Hello, 👋
The transition into menopause is often discussed in whispers, focused primarily on managing "nuisance" symptoms like hot flashes or night sweats. However, for the longevity-minded individual, this period—spanning roughly your mid 30s to mid-50s—represents something far more significant. It is a Longevity Window, a physiological pivot point that heavily influences your health trajectory for the next decades.
A crucial note on focus: This guide dedicates a significant amount of space to Hormone Replacement Therapy (HRT) also called Menopausal Hormone Therapy (MHT). This is not because hormones are the single most important factor in longevity, but because women are historically under-informed, misinformed, or dismissed regarding HRT. We want to close that information gap. Nevertheless, lifestyle is your ultimate foundation. You cannot out-prescribe a poor diet, a sedentary lifestyle, or chronic sleep deprivation. Hormone therapy is the shield; your lifestyle is the armor.
To be precise: Menopause is actually just one day—the day marking exactly one year since your last absent period. The very next day, you are in postmenopause. Perimenopause, however, typically starts 4 to 8 years prior (often in your mid-to-late 40s). It is a phase of intense hormonal roller coasters, and this is when the physiological recalibration begins.

Dr. Maya Fehling is a physician, entrepreneur, and digital health expert working at the intersection of clinical medicine and preventive technology. She currently serves as Co-Founder and Chief Medical Officer of The Longevity Practice, where she leads the development of evidence-based clinical protocols with a focus on gender-based longevity and personalized healthspan optimization.
Her career began in global health with Doctors Without Borders and as a Harvard Global Health Leadership Fellow, where she saw firsthand how preventive medicine and technology can close the gaps left by traditional healthcare systems.
She has also founded a women’s health startup, bringing hands-on experience in user-centric design and targeted health communication. Maya is a frequent speaker and ecosystem connector in Germany’s digital health landscape.
A common desire is to navigate menopause "naturally." While this is a completely valid feeling, it is crucial to recognize that from an evolutionary perspective, "natural" is rarely "optimal.”
Biology's primary goal is reproduction. Once that window closes, evolutionary pressure drops. To conserve resources, the body stops investing energy in physiological upkeep, leading to the "natural" degradation of bone, muscle, and vascular health. Nature's plan is simply to save energy for the next generation.
Furthermore, modern life is already wonderfully "unnatural." We take antibiotics to survive infections, drive cars, and expect to live decades past historical lifespans. Enduring severe menopausal symptoms or skyrocketing chronic disease risks just to remain "natural" is a misplaced badge of honor.
Longevity medicine elegantly "tricks" the body into believing it is still in its vital, reproductive prime. By restoring hormones and using targeted lifestyle interventions, we send a powerful signal that the body is still worth investing energy in—actively choosing optimal vitality over natural decline.
During premenopause, your endocrine system operates in a rhythmic, predictable cycle. As you enter perimenopause, this stability vanishes, resulting in a systemic shift that impacts every major organ system. To truly understand this transition, you have to look at the communication loop between your brain and your ovaries.
To visualize this profound transition, look at the visual comparison below, contrasting the highly cyclical nature of premenopause with the chaotic fluctuations of perimenopause, before everything eventually flatlines in postmenopause.

FSH (Follicle-Stimulating Hormone) & LH (Luteinizing Hormone): These are the "messenger" hormones sent from your brain (the pituitary gland) to direct your ovaries. FSH tells your ovaries to produce estrogen and mature an egg, while LH triggers ovulation. As you reach early-to-mid perimenopause, your aging ovaries become less responsive to these signals. Sensing the fluctuating estrogen, your brain tries to compensate by "shouting" louder—pumping out progressively higher levels of FSH to encourage the ovaries into action. Therefore, a rising or erratic FSH level can be a clinical indicator that your ovaries are struggling to respond and your ovarian reserve is depleting.
Estrogen (E2, Estradiol): Rather than a graceful, linear decline, estrogen becomes highly volatile in perimenopause. It experiences dramatic spikes and steep drops before eventually remaining consistently low.
Progesterone: This hormone offers a natural calming, neuroprotective effect. It typically begins a steady decline in your late 30s or early 40s. Because progesterone is primarily produced after you successfully release an egg, less frequent ovulation means a significant reduction in progesterone.
Testosterone: Unlike the roller coaster of estrogen, testosterone does not suddenly drop during perimenopause; rather, it generally declines slowly and steadily starting in your 20s.
In longevity medicine, the focus is on the primary drivers of mortality. The hormonal shifts of perimenopause act as an accelerant for these key risks:
Estrogen is a master regulator of vascular health. It stimulates the production of nitric oxide, which keeps blood vessels relaxed and flexible. As estrogen declines, this vasoprotective effect vanishes. Arteries stiffen, endothelial function degrades, and baseline blood pressure often creeps upward. Simultaneously, your lipid metabolism alters: your liver produces more LDL (the "bad" cholesterol) and ApoB, while HDL loses some of its protective, anti-inflammatory functions. This perfect storm of stiffer arteries and a deteriorating lipid profile is why a woman’s risk for heart disease—the number one killer of women—sharply accelerates after menopause.
Menopause is a neurological transition just as much as an ovarian one. The female brain is packed with estrogen receptors, and estrogen actively pushes the brain to burn glucose for energy. As hormones fluctuate and drop, the brain experiences a temporary "energy crisis," struggling to efficiently use glucose. This manifests clinically as "brain fog," memory stuttering, word-retrieval issues, and severe mood swings or new-onset anxiety. Furthermore, the loss of estrogen impacts neuroplasticity and serotonin production. While estrogen profoundly supports transition symptoms and general brain health, it is not currently prescribed as a guaranteed shield for Alzheimer's disease prevention, studies are ongoing*.*
It is not just your imagination; your body composition actively works against you during this pivot. Estrogen directs fat storage to the hips and thighs (subcutaneous fat). Without it, fat storage aggressively shifts to the abdomen as visceral fat. This isn't just cosmetic; visceral fat is a highly active, toxic endocrine organ that constantly secreting inflammatory cytokines. This shift directly impairs how your cells respond to insulin, driving up your HOMA-IR and fasting insulin scores, and drastically increasing the risk for metabolic syndrome and Type 2 diabetes, even if your diet and scale weight haven't changed.
Bone is living tissue, constantly being broken down by cells called osteoclasts and rebuilt by osteoblasts. Estrogen is the master brake on osteoclasts. When estrogen plummets, that brake is released, and bone breakdown rapidly outpaces bone building. Women can lose up to 10% of their bone mass in the first five years after menopause alone. This degrades the actual microstructural integrity of the bone, leading to osteopenia and osteoporosis. For context, for those over 65, a hip fracture carries a staggering 25% mortality rate within one year.
Estrogen is a potent, natural anti-inflammatory agent. Its withdrawal tips the entire immune system into a state of chronic, low-grade, systemic inflammation. Pro-inflammatory cytokines (like IL-6, TNF-alpha, and hs-CRP) spike. This "inflammaging" accelerates the breakdown of joint cartilage (explaining sudden, severe menopausal joint pain), degrades the gut microbiome barrier, and acts as the underlying fire that fuels cardiovascular disease, neurodegeneration, and cancer.
Breast Cancer: Research suggests the absolute risk increase from certain older HRT is roughly 0.1%—lower than the risk associated with moderate alcohol consumption. Modern data links this risk primarily to older synthetic progestins, not bioidentical progesterone.
Endometrial Cancer: Taking estrogen alone increases uterine cancer risk. Using progesterone is mandatory for anyone with a uterus to neutralize this risk.
The Obesity Link: Overweight and obesity are major risk factors for cancer. If HRT, combined with lifestyle, mitigates menopausal visceral fat accumulation, it indirectly targets a major driver of cancer risk.
Evidence suggests there is a "Critical Window" for starting HRT—ideally within 10 years of menopause onset and before age 60. Taking action within this window offers the greatest cardiovascular and neuroprotective benefits.
However, the decision of exactly when to start should be symptom-oriented, and you do not need to wait for your periods to stop. The symptoms of perimenopause are systemic and frequently misdiagnosed as general aging or stress. If you are experiencing a cluster of these issues, it is time to start talking to your doctor: classic hot flashes and night sweats, trouble staying asleep, severe joint and muscle pain (like "frozen shoulder"), brain fog, uncharacteristic irritability, new-onset anxiety, or a plummeting libido.
In many countries (including Germany), HRT products are officially approved specifically for postmenopause. Prescribing them for perimenopausal symptoms is common practice but technically "off-label." If your symptoms are dismissed, do not give up. Consider seeking a second opinion from a gynecologist or endocrinologist who specializes in menopause or longevity medicine.
Transdermal Estrogen (Estradiol, E2): Delivered via patches, gels, or sprays, this method bypasses the liver, heavily minimizing the risks of blood clots and stroke associated with older oral estrogen pills. Estrogen thickens the uterine lining. If you have a uterus, estrogen must be paired with progesterone to prevent unchecked cellular growth (endometrial hyperplasia), which increases the risk of endometrial cancer.
Micronized Progesterone: This is the bioidentical standard. It safely stabilizes and protects the uterine lining while significantly improving sleep architecture. If oral progesterone causes severe grogginess, the capsules can often be used vaginally to bypass the digestive system.
Transdermal Testosterone: While transdermal estrogen avoids the testosterone-crashing side effects of older oral pills, your natural testosterone levels still decline steadily with age. Therefore, transdermal testosterone supplementation should be discussed as a core component of HRT to support muscle mass, energy levels, and libido. (Rest assured, physiological, female-dosed testosterone simply restores your 20-something baseline—it will not cause you to grow a beard or sound like a lumberjack).
Standard HRT is not birth control; you can still get pregnant. While some doctors offer the standard birth control pill to manage perimenopause, longevity medicine strongly prefers transdermal HRT. Birth control completely shuts down your natural ovarian production with high-dose synthetic hormones, whereas HRT gently supplements your declining natural hormones.
In longevity medicine, the current practice is often "never"—continuing therapy indefinitely to maintain lifelong cardiovascular, cognitive, and bone protection, provided your ongoing health screenings remain clear.
While diagnosing perimenopause is symptom-based, testing provides a crucial baseline to understand your unique physiology.
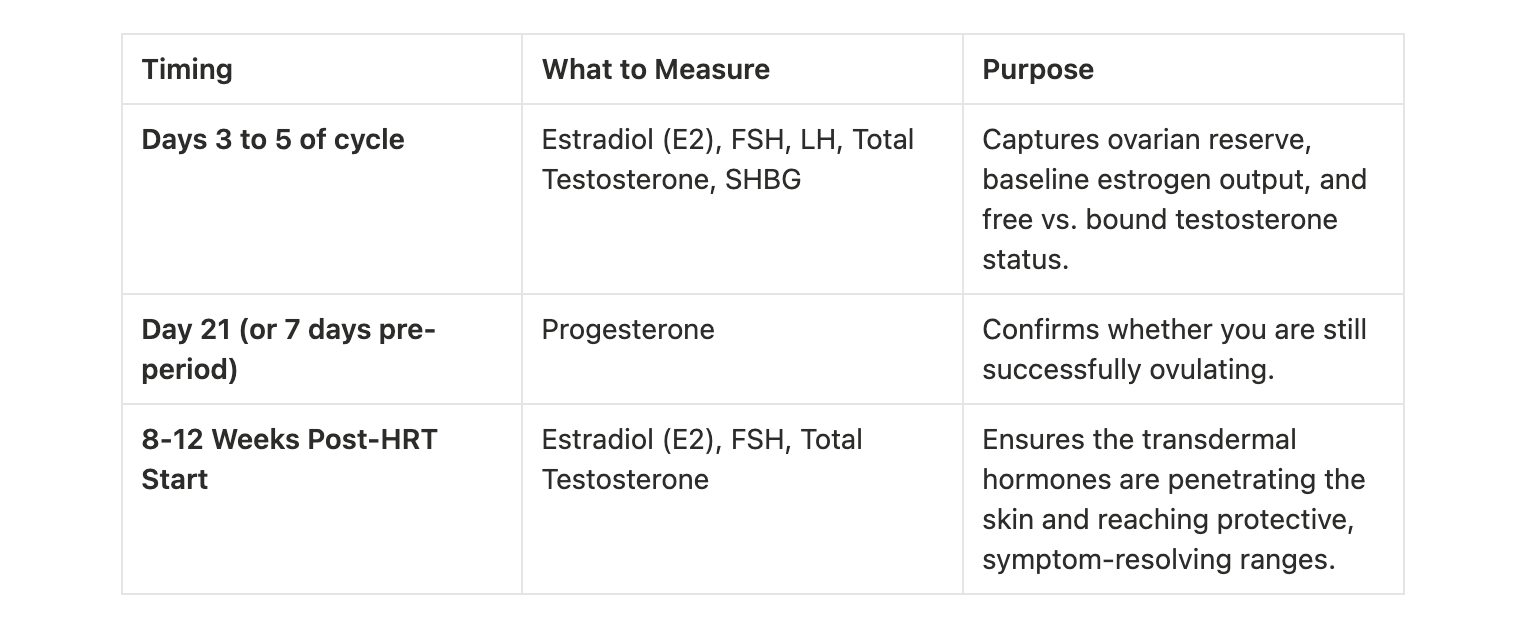
(Note: If your cycles are totally erratic and Day 21 is impossible to predict, work with your doctor to pull a general baseline on a day you are experiencing a surge in symptoms).
HRT is a fantastic tool that optimizes your biology so your lifestyle interventions can work more efficiently. However, HRT is not an option or a desire for everyone. Whether by personal choice or due to strict medical contraindications (such as an active or recent history of hormone-receptor-positive breast cancer), you are not powerless. If HRT is off the table, aggressive lifestyle interventions become your primary, highly effective shield against age-related decline.
For too long, the cultural narrative around menopause has been one of loss, decline, and quiet endurance. It is time to completely rewrite that script. Perimenopause is not an ending—it is a physiological wake-up call and a profound opportunity to finally put your own health, strength, and longevity front and center.
This begins with a radical identity shift. Instead of accepting the old narrative that your body is starting to decay or fail you, adopt a new one: "I am stepping into my most unapologetic chapter. My body is recalibrating, and I am actively building an optimized, resilient foundation for the next forty years."
Menopause is not a fading away; it is a distillation. The physiological fire of this transition burns off what no longer serves you, leaving behind a stronger, wiser, and highly capable version of yourself.
You now have the roadmap, the science, and the tools. The next decades are entirely yours to define—armor up, and make them your strongest yet.
 EN
EN
 DE
DE
